Testosterone and immune
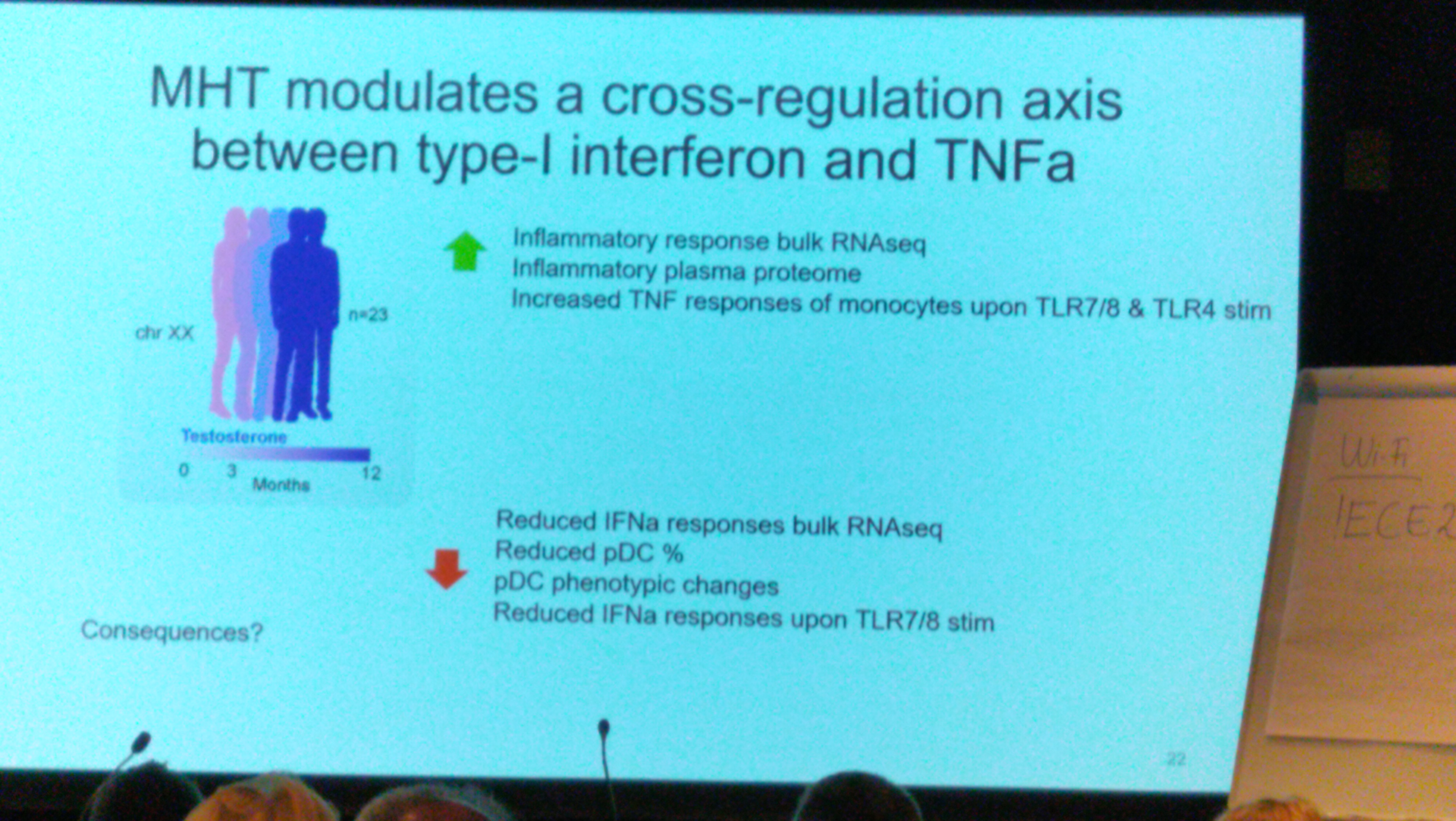
Masculinizing hormone therapy
n=23 XX — 0-12 month
Profile immune system by
- Mass cytometry
- pDC⬇️ CD141+DC⬆️ MDSC⬇️ Monocytes⬇️
- bulk RNA-seq and scRNA-seq
- IFNa
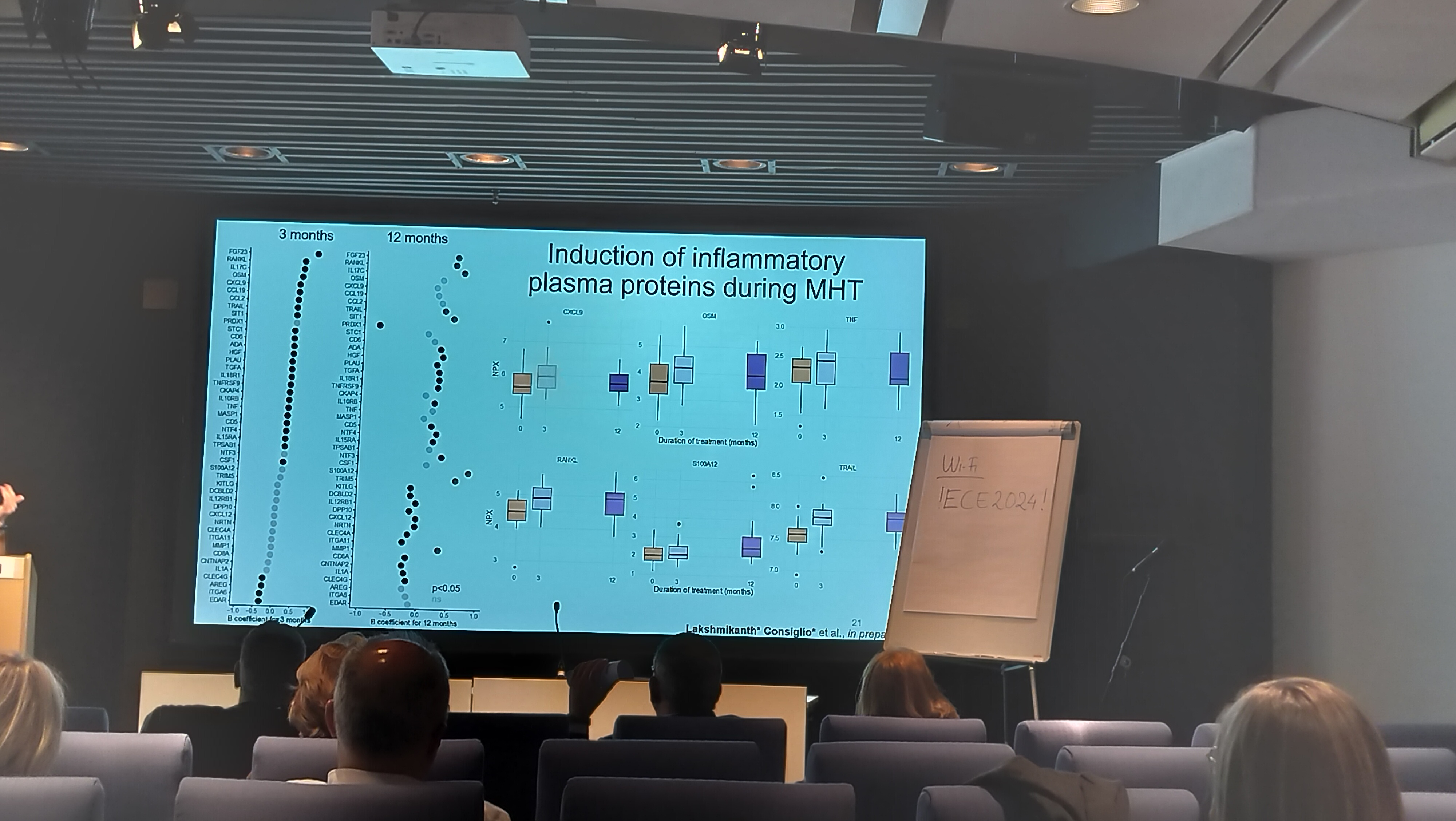
- Olink
- inflammatory: CXCL9, OSM, TNF, RANKL, S100A12, TRAIL
- inflammatory: CXCL9, OSM, TNF, RANKL, S100A12, TRAIL
in-vitro functional test (cellular)
4h TLR7/8 —> scRNA profile
pDC: IFNa ⬇️ , Type-I and Hallmark IFNa
Monocyte: Hallmark IFNa⬇️
PCOS
- low grade inflammation
- asthma
- SARS-COV2, COVID19
n=58 control, n=108 PCOS,
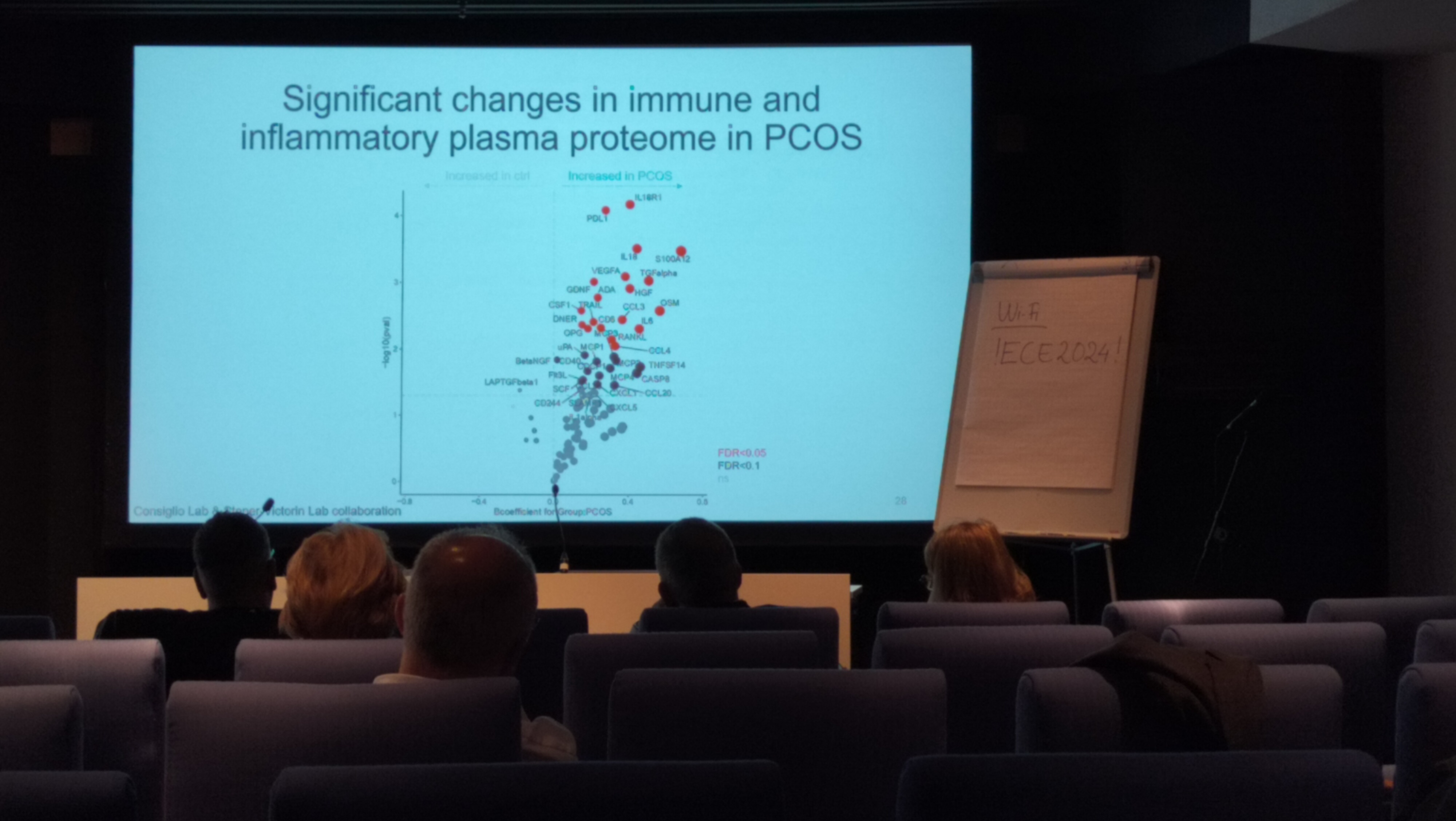
→ Olink
→ metbaolic markers: HOMA_IR, BMI (~CSF1, PDL1), SHBG
→ reproductive markers: testosterone, FGscore, LH
correlation between metabolic and reproductive markers lost in PCOS
testosterone, positive with immune marker in control, negative in PCOS
??cells: CSF1, CCL2,
myeloid cells: IL-6, S100A12, OSM
?? cells: S10A12, OSM
—> IL-18, IL18R1 —> TYPE 1 IMMUNE RESPONSE
—> turning down immune ??
MYELOID CELL ACTIVATION, INFLAMMASOME SIGANLING AND IMMUNE EXHASUTION
QA
Q1: from genetics, testestrone not the driver? Q2: transman vs man Not completely switched
PCOS endometrium
proinflammatory Macrophage <- ?? cell type antiflammatory Macrophage <- ?? cell type
hyperandrogenism –> immune functions –> insulin + xx (androgen?)
mice model: normal weight PCOS
in uterus eosinophil⬇️ (Eotaxin⬇️, IL5 not changed) NK matruation (with markers) ⬆️
Adipose tissue
- eosinophole ⬇️ in visceral adipose tissue
- CD69+ NK ⬇️
- mature NK ⬇️
Testosterone on TLR in transmen
Background
TLR higher in female, TLR7/8 on chrX, GAHT on immune (Gap and Aim)
Methods and results
Prospective observatory study, 21 transmen,
karyotype + RT-PCR for TLRs(8, 10 ⬇️), CD144, MD2 ⬆️
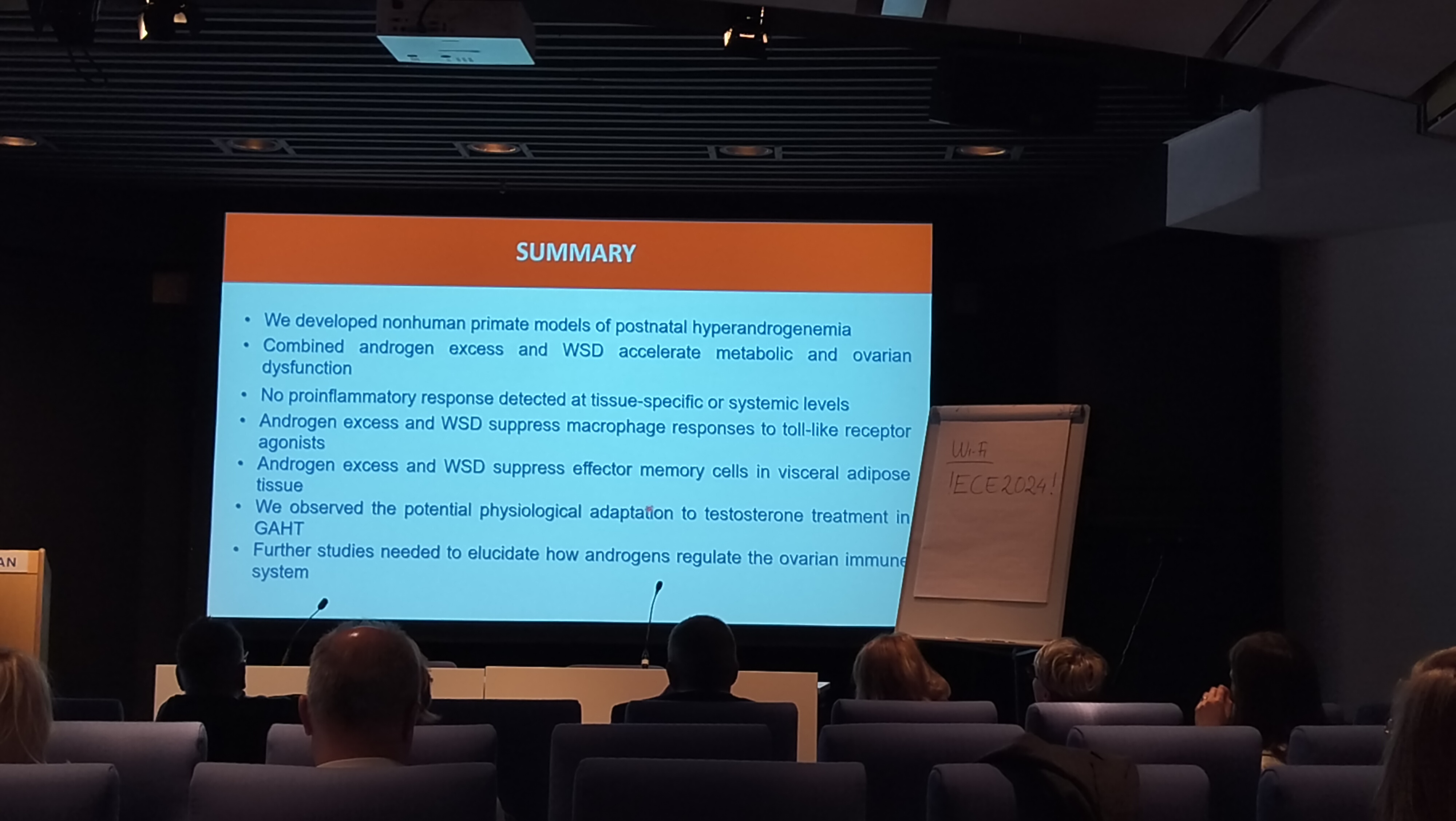
Prepubertal Primate model and Immune function
primate models and metabolism
2.5 yo –> 5.5 yo
- chow
- T+chow
- WSD
- T+WSD
-> fetility trials (util 7yo) -> reversal with chow to 7.5 yo
—- functional dissection – 3 yo treatment (not sig. until 2 yo)
- T+WSD: fasting insulin HOMA-IR BW (BV,VF), FFA update, lipolysis ⬆️
- NOT with individual treatments
- innate immunity and TLRs
– 7 yo treatment and 0.5 yo reverse
another cohort to focus on immune
1 yo treatment (from 6 yo to 7 yo)
- chow
-
T+WSD –> metabolism & immune
- adipocyty% changed
- C-peptide and CCL5 not changed
–> immune cells in peripheral tissues and blood by FC with
- lymphoid surface
- macrophage surface
- TLR stimulation cytokine response NOT significant
–> macrophage response to TLR1/2
control response in IL6⬆️, and %CD11b+HLA-DR+cells
–> T cells not significant changes
–> memory T cells Tn, Tcm, Tem (CD28, CD95) in omental fat, CD8+ effector memory cells ⬇️ by hyperandrogenemia, coor with HOMA-IR in OM-FAT WSD alone does not alter
11-oxygenated androgens in PCOS
chronic kidney disease (Hsd) -> 11-oxygenated androgens⬇️
methods
- oral DHEA (n=10)
- oral 11KA4 (97% purity) (n=10) -> androgen metabolism -> insulin resistance [2-step (low -> high dose insulin) hyperinsulinaemic-euglycaemic clamp]
results
D7:
- DHEA: [classic] A4, T, DHT; DHEA ⬆️, 11KA4: not change
- [11O androgen pathway] 11OHA4, 11KA4, 11OHT, (urinay) 11OHAn, 11OHRt, … ⬆️ in 11KA4, not in DHEA
- insulin resistance, neither changed
QA-p5
- dosage effects
- adipose tissue (no), muscle biopses (on going): data awaited
- clinical concern: androgen to high-androgen pcos women; side effects after D7? three month DHEA before IVF, so probably no side effects with 7 days oral treatment
Kispeptin as a test of hupothalamic function in women with oligo-amenorrhea
Presenter: Bijal Patel
menstrual disturbance (1/5) <- PCOS/HA(hypothalamic amenorrhoea)M- low bw, excessive exercise, ??, ?? difficulty in differentiation
both have divergent hypothalanic function:
GnRh frequency: PCOS: ⬆️, HA: ⬇️
congenital structural aberrance (CHH)
Results from kisspeptin given
kisspeptin-54 9.6nmol/kg: ⬆️LH and FSH in PCOS, the LH response similar to control; FSH reduced compared to control
Influencers by correlation: Inhibin B; AMH obesity increase LH and FSH response
Clinical lean PCOS; different after kispeotin vs HA
My question: discriminate three group AUCROC? PCOS vs CHH?
My guess: too obvious so no need clinically?
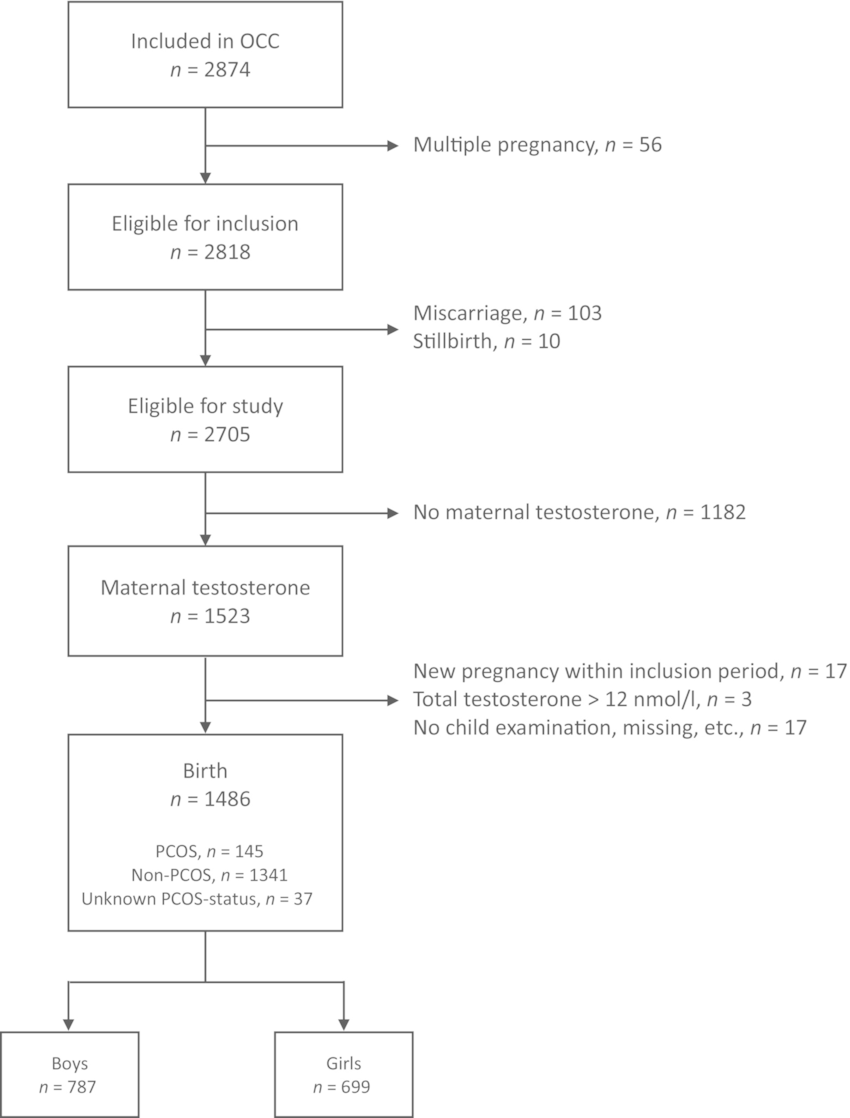
prenatal testosterone and offspring body composition (7yo)
Odense child cohort
 testosterone –> fetus (free testestrone ⬆️ from 3rd trimester)
testosterone –> fetus (free testestrone ⬆️ from 3rd trimester)
monkeys: ⬆️abdominal fat mass in females
- mother: total by LC-MS/MS; free by -SHBG; diagnosis
- children: Fat%
- DAG: factor analysis
results in boys
free testosterone ~ BMI, Fat mass index ⬆️; lean ⬇️
results in girls
NOT as significant in the sig. changes in boys
maternal PCOS ~ gynoid fat%⬇️ only
QA-p7
- why corrected for birth weight, but not taking as interaction
- Androgen/Estrogen ratio
Kidneys in PCOS
renal injury, AR ⬆️-> IL-6⬆️ ->(STAT)-> mitochondra
Other reference: placental stat3
so maybe we could look into IL-6/mitochondra (not feasible in the current project but future) in our PCOS project?
mice experiment
- veh
- pcos (DHT): IL-6, JAK1/2, STAT ⬆️, STAT inhibitors⬇️
- STAT3 inhibitor
- normal levels in the aforementioned expression
- complex I, II, III, IV-; mtROS -> mitochondra dysfunction restore
- renal injury restore
cellular experiments
DHT on renal cells
immune-metabolism and pregnancy loss
Tregs - uNK
Tregs deficiency in early pregnancy failure (EPF)
- %Trreg/CD$+T
- CTLA+ (suppressive marker)
- /Th1 and /Th17
EPF upregulated in Treg pro-inflammatory 1/4 are FOXP3 targets
Q: if cellular abundance lower but transcription abundance increase; so much more increased from the cells?
Insulin/glycemic <–> inflammmation/immune tolerance
fasting and OGTT at 6w mid-phase post-miscarriage (at least 2 times, n=64) & T cell
- HOMA-IR ⬆️ (insulin resistance)
- not alter CD4+ & CD8+ T cell abundance, not Treg neither
- reduce HLADR+CTLA4+HELLOs+ (suppressive markers)
- reduce proliferating Treg (Ki67)
- increase naive CCR7+CD45RA+ Treg
- reduce central memory and effector memory Treg with genetically normal fetuses
targeted therapies
cluster of patients with immune and metabolic dysregulation
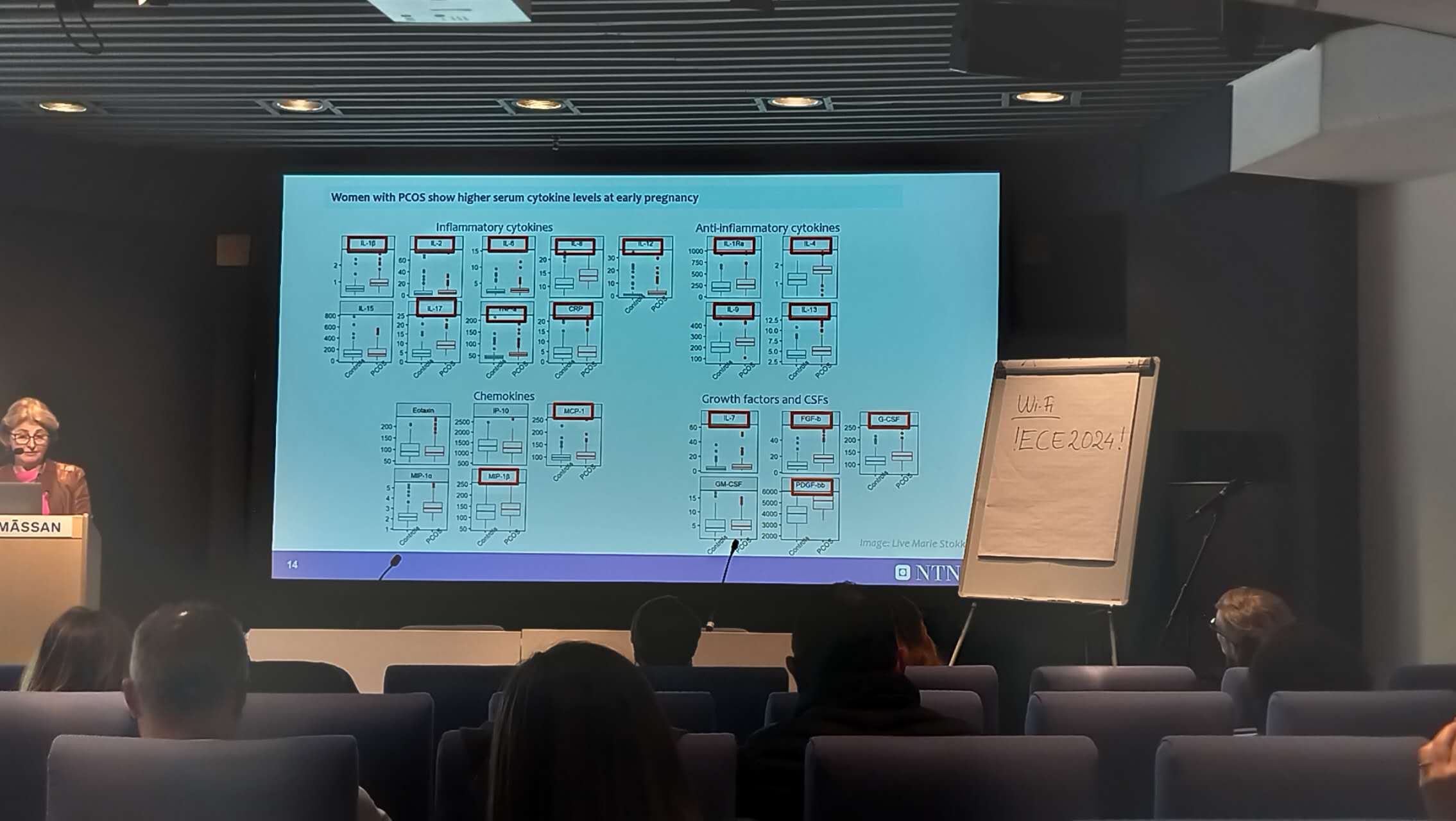
cytokines in PCOS pregnancy
presenter: Eszter Vanky
immune develppment in PCOS vs. normal
- Normal (n=258):inflammation –> anti –> inflammation
- PCOS (n=358)
 inflammatory and growth cytokines
inflammatory and growth cytokines
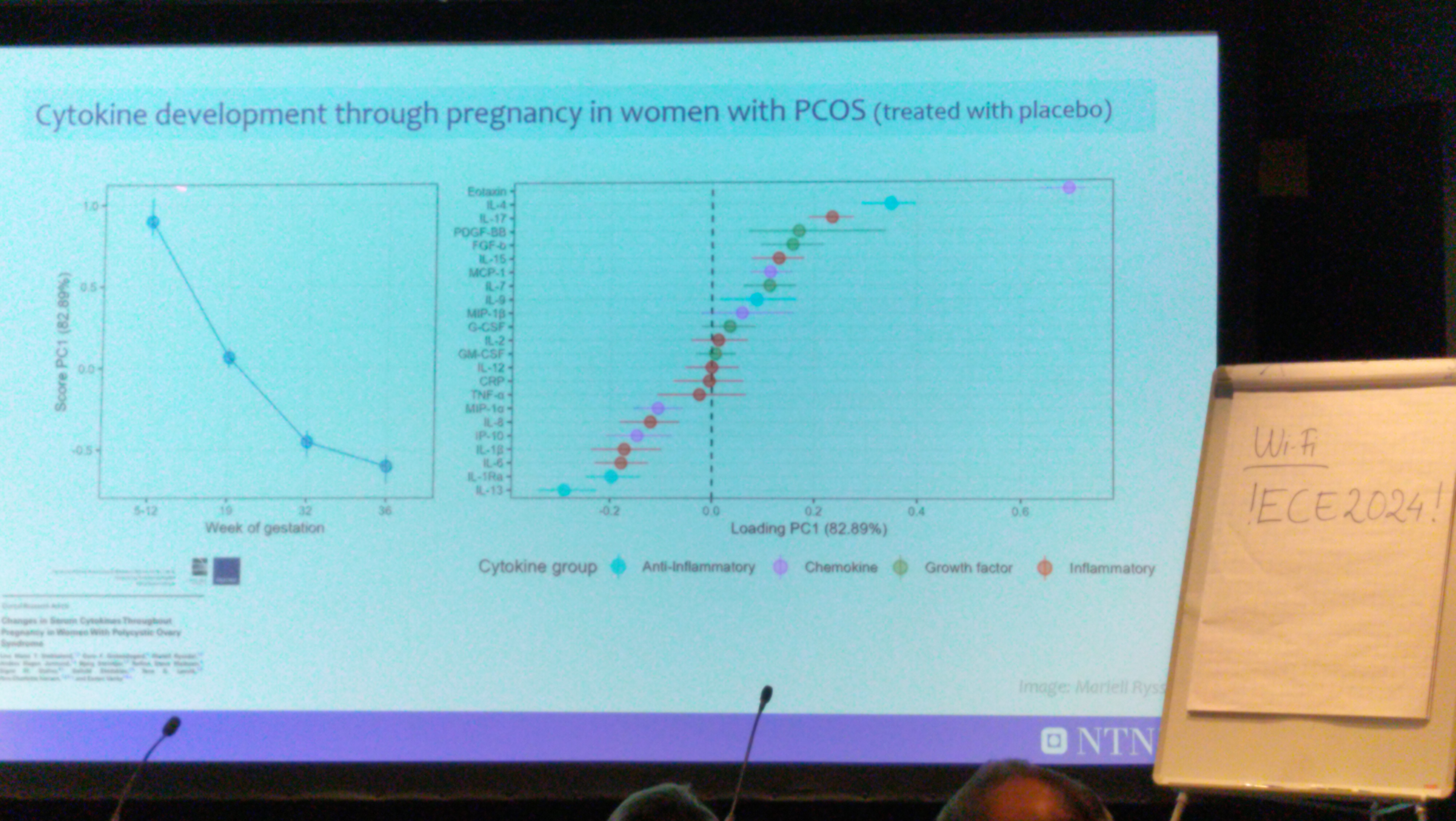
 In PCOS-placebo
Score PC1, contributors: Eolaxin, IL-4, IL-17, PDGF-BB, FGF-b (decrease through pregnancy); IL-13, IL-IRa, … (increase through pregnancy)
In PCOS-placebo
Score PC1, contributors: Eolaxin, IL-4, IL-17, PDGF-BB, FGF-b (decrease through pregnancy); IL-13, IL-IRa, … (increase through pregnancy)
 Also with mobility analysis
Also with mobility analysis - overweight/obesity
- IL-IRa
- CRP
- hyperandrogenism
- FGF-b
- IL-2
- IL-16
- IL-8
- fetal sex
- meta-analysis with >12m individuals: male more PE and preterm
- metformin
- increase immune, eolaxin, FGF-b, IL-17, IL-4, …
- less viral infection and allover infection
- children at 7 yo
- higher allergy and eczema from metformin
Now I have controlled fetal sex, or maternal BMI, two batches of analysis; but not both of them. Maybe I should just try one batch with both controlled.
In combination with our data, probably the effects to the offspring could be directly to the fetus, not really from placenta.
QA-Estzer
- 80% compliance for dosage (2.5g)
- insulin resistence ~ allergy: randomized controlled study, so the mechanism causes are random, no cause-effect from other factors
- concentration in the umbinical cord is the same in the the maternal serum
- placenta is highly vascularized so small molecules can accumulate
- leaky placentas
we have the results for the prior usage of metformin, it’s better to put them in hidden slides and answer the questions
-
Previous
Algernon: outside of the boundary of human science and ethics -
Next
Introduction the speakers at Epigenetic Symposium